
NOTE: This is the culmination of Zen and the Art and Science of Immersive Storytelling: A Unified Theory of Narrative Engagement, which recursively applies the theory to real-world experience. Earlier essays discussing the theory at length can all be found here.
Many companies put a premium on both safety and quality in their workplaces. The two do not have to be mutually exclusive, and, in fact, go hand in hand. As someone who has worked for some of the top companies in their fields, that accomplished unprecedented results, as well as another that maintained a level of mediocrity, I can attest to this being true.
The difference in outcomes was a stark lesson in how one organization successfully integrated both, while the other was an informal case study in the consequences of their separation. A true understanding of their differences remained elusive until recursively examined through the lens of the Unified Theory of Narrative Engagement. The theory not only demonstrated how organizations have their own narratives, but also how it can pinpoint where, why, and how things went awry.
But first, let’s set the table.
When an accident occurs — or, in some cases, an incident — a formal investigation is often undertaken to discover the root cause and associated causal factors. The team assembled becomes detectives, trying to piece together a puzzle with a myriad of diagnostic tools. They are, in essence, reverse-engineering a specific genre of story: a mystery.
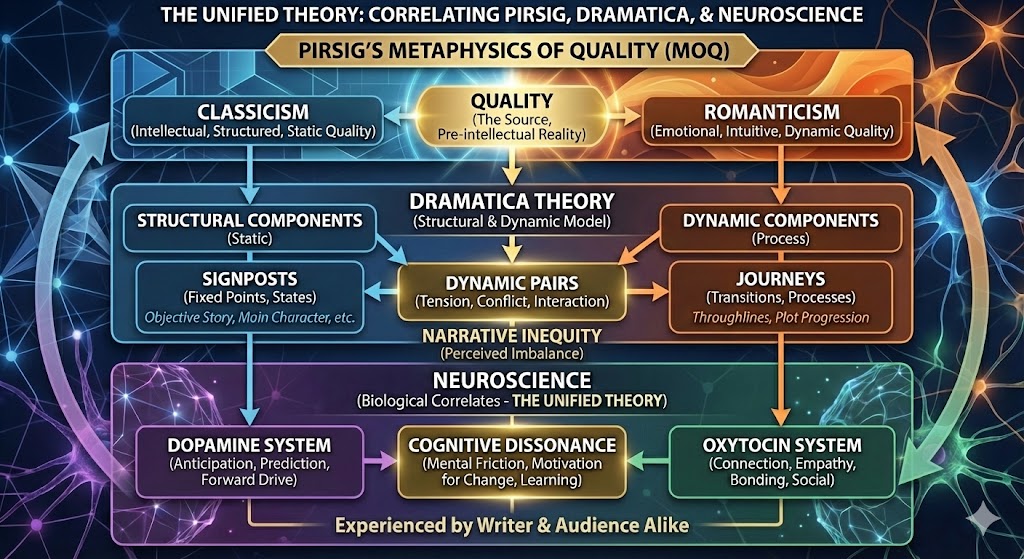
The tools, data, directives, procedures, and processes are to be explored as examples of Pirsig’s Classicism at work. This is what most investigations focus on. Did the operator follow the procedure? Was the part manufactured to spec? They are the tangible, analytical, yet Static Quality components of the system — but an investigation that stops here only identifies the what, not the why, and this is where Pirsig’s idea of Romanticism comes into play.
The principles of effective communication in high-stakes environments, such as those outlined in the book Crucial Conversations, offer a practical lens. The authors note that when stakes are high, we are often at our worst, and the first step toward a productive outcome is to “Start from the heart.”
This principle is a direct, actionable parallel to Pirsig’s notion of “Care.” It demands that we first examine our own motives and what we truly want for ourselves, for others, and for the relationship. By focusing on “me” first, we shift from a Classical, analytical mode of assigning blame (“you did this”) to a Romantic, holistic mode of seeking mutual understanding. This shift is crucial for fostering the psychological safetynecessary for honest dialogue to occur.
This sense of “Care,” or starting from the heart, must permeate the entire organization in an effort to get everyone rowing in the same direction. Without it, underlying issues such as lack of engagement, schedule over safety, and poor accountability can create an absence of Quality. This void is quickly filled by Cognitive Dissonance, leading to a passive-aggressive workforce willing only to do the bare minimum, if they’re not already completely tuned out.
Healthy organizational cultures maintain a neurochemical balance at scale: Oxytocin (Romanticism) fosters trust and cohesion; Dopamine (Classicism) rewards productive anticipation and achievement. But when these forces fall out of harmony, when reward becomes detached from care, the resulting dissonance is not merely emotional — it’s systemic.
Most of the time, employees understand the company’s goals and expectations. Yet they experience cognitive dissonance when they’re told one thing, then see leads, supervisors, and managers disregard principles the company itself says it values most.
A seed of disharmony is planted and takes root as a result. Employees begin to talk. Soon, it’s “us vs. them,” mirroring Dramatica’s four throughlines of perspective, and “Care” is a four-letter word preceded by the words, “I” and “Don’t.” And when people don’t care, all the classicism in the world in the form of procedures, safety manuals, training, etc., suddenly loses meaning, turning a work culture ripe with risk factors for an accident.
Dr. Paul J. Zak’s research provides the biological mechanism for why this is so corrosive. High stress and uncertainty are potent oxytocin inhibitors. The chronic cognitive dissonance, being told one thing while seeing another, is a significant source of workplace stress.
This creates a devastating feedback loop:
Dr. Zak’s Trust Factor isn’t just diagnostic; it prescribes. His OXYTOCIN acronym is a set of actionable behaviors that stimulate the release of oxytocin, build trust, and, in essence, rewrite a company’s broken story.
Ovation (recognize high performers)
Xpectation (set clear, challenging goals)
Yield (grant autonomy)
Transfer (enable self-management)
Openness (share information transparently)
Caring (intentionally build relationships)
Invest (promote growth)
Natural (be authentic and vulnerable)
And there are even more ways of diagnosing issues: applying Dramatica’s four throughlines of Story Mind perspective to an accident investigation, we might see something that looks like this:
The Objective Story (They): This is the sequence of events, the “what happened.” It’s the timeline of mechanical failures, human errors, and environmental conditions that affected everyone involved. This is the domain of “root cause analysis,” but it’s only one-quarter of the story playing out like a mystery.
The Main Character (I): This perspective could be embodied by the investigator, who moves from a state of not knowing to a final understanding. More powerfully, it could be the perspective of a key employee, the one who felt the unease, who saw the cracks, who lived with and experienced the dissonance. Their internal journey (“I’m being told safety is the priority, but I feel pressured to take shortcuts”) is the subjective heart of the story.
The Influence Character (You): This is the opposing worldview. It could be a specific manager, but it’s more likely the organizational culture itself, personified. This is the voice that says, “You have to make the deadline,” “Don’t worry, it’s always been done this way,” or “We can’t afford to slow down.” This perspective relentlessly pressures the Main Character (the employee) to abandon their “care” in favor of expediency.
The Relationship Story (We): This is the core conflict between the stated values and the practiced values. It’s the story of the relationship between the workforce and management. Is it built on trust and mutual care, or on suspicion and competing priorities? The breakdown of this relationship, the growing gap between “what they say” and “what they do,” is where the true story of the accident unfolds.
An investigation that fails to map all four of these throughlines will produce an incomplete story, and therefore, an incomplete understanding of the accident. It will blame a single part or a single person (the Objective Story) without understanding the psychological pressures (the MC/IC conflict) and the systemic breakdown of trust (the Relationship Story) that made the failure inevitable.
When employees are told, “We care about your safety,” but are rewarded (or not disciplined) for actions that compromise safety, they are placed in a state of profound cognitive dissonance.
This isn’t just an uncomfortable feeling; it’s a powerful motivational state that the brain is desperate to resolve. As noted, employees know the expectations, but see conflicting evidence. To reduce this dissonance, they must do one of three things:
In a culture where “care” is absent, the path of least resistance is always 2 and 3. This leads to a systemic erosion of trust (an oxytocin deficit) and a realignment of the reward system (dopamine) toward the rewarded behavior (speed) rather than the stated value (safety). The dissonance doesn’t just create disharmony; it actively rewires the organization’s operational morality.
The final accident report, the “story told in reverse,” is the ultimate, tragic resolution of that dissonance. This theory provides the framework to not just document the failure, but to diagnose the exact point where the organization’s “Engagement Field” broke, where the absence of romantic “care” made the classical procedures meaningless.
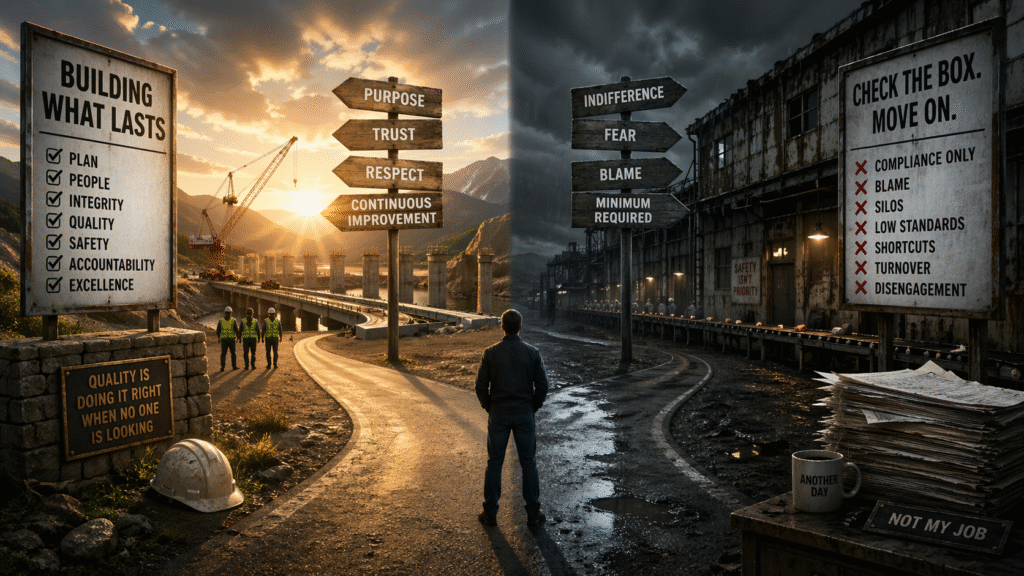
Every organization tells a story. When its words and actions diverge, the narrative fractures, and people stop believing in the protagonist. Rebuilding safety is not about rewriting procedures, but restoring coherence between belief, action, and care.
That coherence is what Pirsig called Quality. Let’s take a real-world example of what this looks like, the Unified Theory in full recursive action as I reflect upon my own lived experience.
What follows is not a memoir. It is a real-world case study of an organization unknowingly operating according to the principles of the Unified Theory years before the theory existed.
From 2001 to 2009, I worked for a partnership between two prestigious companies in the top ranks of their respective fields: Bechtel and SAIC. Bechtel SAIC, or BSC, as it was known, was the management and operating contractor chosen for the Department of Energy’s Yucca Mountain Project, based approximately 90 miles north of Las Vegas, NV, at the then-named Nuclear Test Site, with offices in Las Vegas and Washington, D.C.

My story’s inciting incident here began with a near miss submitted through the project’s Corrective Action Program due to an incident in Las Vegas, when transferring servers to the campus from the warehouse. A lift-gate malfunction nearly resulted in injury and significant property damage. The near miss resulted in a stand-down on moving items until a full review was completed.
The result: I was put in charge of turning a customer service desk into a Work Control unit. Entire procedures and JSAs needed to be rewritten, but during this, as a moment of upheaval and change, I saw the opportunity to rewrite the entire process, including workflow, tools, and software, integrating them all into a value-driven, Computer Aided Facility Management System (CAFM), to include a paperless Work Request system with a satisfaction survey for continuous improvement.
This wasn’t just a technical upgrade; it was the automation and formalization of a feedback loop as a structural commitment that conveyed, “Your voice matters and helps us to continually improve.” As an oxytocin-inducing principle, this moved from co-authorship of a new process to co-partnership and a stake in its and the project’s future success, with each feedback providing the same opportunity as the originating corrective action.
This wasn’t accomplished in a vacuum: it required assistance and coordination from numerous departments, from business case and requirements document to sole-source justification and request for proposals, selection, and awarding.
During this time, I took the opportunity to invite the most vocal of our department’s critics — those who actively used the Corrective Action Program and provided critical feedback on the prior work processes — to come to a meeting where I explained what I was about to do, why I was doing it, and why I needed their help.
I was, in essence, turning them into stakeholders by giving them a seat at the table, knowing that if I could get their buy and and support, I would have achieved a level of Pirsig’s Quality that had been absent.
Only in recent reflection, as part of developing this theory, did I realize: A healthy organization treats productive dissonance, what was experienced via the “vocal critics,” as a resource and opportunity rather than a threat that needed dismissal.
The biggest critics were the people experiencing the most dissonance between the system as it existed and the system as it should have been. They were already engaged enough to complain, already invested enough to be frustrated. Meeting with them was where the romantic element entered. The system could have been built without them and their input, but building it with them, turning their dissatisfaction into investment, their frustration into ownership, is what made it a Quality achievement rather than just an efficient one.
By giving them a seat at the table, I unknowingly did something neurochemically precise, transforming their dopamine loop from anticipation of failure, the cynical expectation that nothing would change, which is itself a form of engagement, just inverted, into anticipation of potential success.
As a result, I also established an oxytocin bond between them and the outcome by giving them ownership of it. If it succeeded, it’s partly theirs, and, as discussed in earlier chapters, they become co-authors of that success.
Most managers treat that energy as resistance to be overcome. I happened to recognize it as the most valuable resource in the room. This is what Quality looks like as operational practice and an example of Dynamic Quality as leadership practice. It was also the direct opposite of what I experienced in our forthcoming and negative example.
The results of this effort, which at the time cost over $200,000 to implement, were the reduction of 1.5 FTEs, over $2,000,000 in a Six Sigma Black Belt project savings, and improvements in overall satfisfaction, real-time data, reduction in work order backlogs, and expediency: a 48-hour goal for assigning a work plan to a request turned into work being completed in less than 24 hours. What wasn’t apparent then, but is now, was that expedience and promptness provided a dividend: Trust.
These were all “Classicist” attributes from Pirsig’s Metaphysics of Quality; the structural underpinnings of getting an organization to function effectively and efficiently, like his symbolic motorcycle in Zen and the Art of Motorcycle Maintenance.
It was here, at the YMP, that I began thinking that the book would somehow make an excellent tool for management; I just didn’t know how. What I seemed to intuitively know at the time, however, was that I only had one part of the equation, the Classicism, in place. The Romanticism portion, the Oxytocin connection, empathy, and care, would come in tandem, and in true Pirsigian fashion, preceded my understanding of it at the time.
All of the achievements to this point were secondary to the purpose, the main goal: the company’s Zero Accident Philosophy. In order to achieve this, it was important to care about what we were trying to accomplish. This entailed designing and building trust and cohesion into the new process and tools. Without those, there would be no buy-in or support.
At the time, I intuitively knew that if people didn’t believe in the process, if the process didn’t meet or exceed their expectations, it would be quietly abandoned. This is what I explicitly told a plant manager years later, which hints at the second portion of the case study, when it was apparent his same processes were broken.
The “living field” between the newly created CAFM and the Work Control process and the robust Corrective Action Program was the Job Safety Analyses. What was accomplished in hindsight of the Unified Theory is a formal organizational instantiation of the theory’s recursive realization principle, a system where a corrective action, the dissonance between expectation and the reality of a different outcome, became the opportunity where “a stumble prevents a fall.”
Each corrective action fed into the system, at the very lowest level, was considered an opportunity for improvement; that was the standard for the Corrective Action Program. Those opportunities may result in the review of a process, a procedure, or a JSA; a recursive process where every corrective action was a prediction error that fed back into the system and updated its model.
That’s an organization designed to function like a healthy narrative; one that incorporates new information rather than defending against it, that treats dissonance as productive rather than threatening, that allows Dynamic Quality to continuously update Static Quality rather than letting Static Quality calcify into meaningless procedure.
As for the JSAs, I began modeling, a form of mirroring and behavioral learning, what I had researched in other effective programs. Specifically, adding risk management into the equation, as that was one of the areas I saw lacking in the original corrective action from the faulty lift-gate. The work entailed the cooperation of multiple organizations: IT, Facilities, Property Management, and the Warehouse, and exposed the lack of coordination between them, which should have signaled an increase in the risk involved.
By adding the equation, Severity of Risk (SoR), and multiplying it by the Likelihood of Event (LoE), I could at least be given a value where the threshold of risk would signal, “Hey, we need to stop and think this one over,” — the equivalent of sitting with one’s dissonance — especially in the event of new and/or unusual work. In fact, the JSAs’ Risk Assessment, when reviewed by Safety, had them questioning why it wasn’t being used at the Test Site.
Since I was starting this from scratch, the values assigned on a scale of 1 to 5 would start as discretionary and based on available industry data, with the intent of being part of the recursive, Dynamic Quality process, where they were continually updated based on corrective actions and Lessons Learned created as action items for their closure.
As a result, a corrective action could generate a Lessons Learned, a form of recursive learning, which then would be added to the applicable JSA, fulfilling the role as both an administrative control and training aid/safety topic. The JSA subsequently became a robust document itself, which could be attached to the work orders and accessed on mobile devices (mind you, this was c.2004).
The result: we had no accidents for several years, equating to over 6 million hours, if not more. I had, several years ago, reached out to the Safety Manager at the time the project was shuttered, but he couldn’t recall the exact number, either. And honestly, that’s the way Quality sometimes works: it becomes so ingrained in the individuals and the organization that it is the standard, because it’s ingrained Classically into the processes themselves.
Bechtel SAIC was subsequently awarded multiple Voluntary Protection Program Star Status Awards and became one of only two Department of Energy Legacy of Star Awards from OSHA.
More importantly, these numbers were mostly achieved during the last half-decade of the Yucca Mountain Project’s existence, when budget cuts and layoffs resulted in a 75% staff reduction under my department alone. Despite this, the Quality and Safety standards remained the same, in both expectation and achievement. Had these changes not been implemented when they were, I don’t believe these results would have been achieved.
In the end, nobody told me how to go about doing any of this or how to achieve it. I followed my own “Romantic” intuition, integrating “what could be” with the “Classical” burgeoning technological aspect to give it form and order. The one thing I believed contributed greatly was my own guiding principle:
“If we can’t demonstrate that we can work safely and efficiently in a large, campus office setting, how can we ever convince the public that we can handle and transport nuclear waste with the required — and expected — level of care it demands?”
What I just provided was, in essence, a demonstration of how involved I was with implementing these processes, procedures and tools that resulted from a single near miss. What they don’t express, however, is to what level I was engaged.
First and foremost, none of this would have been possible without trust. Management saw something in me in a short period of time after the project transitioned, from TRW to Bechtel SAIC, to believe I was capable of accomplishing this. My “boss’s boss,” in fact, once said the only thing she didn’t know whether I could do or not was fly an airplane. Incidentally, my father earned his pilot’s license at the age of 15 by completing a solo flight back in 1945 — before he obtained a driver’s license.
That trust (Oxytocin) resulted in my engagement from the start. Every day I went to work, time passed effortlessly, and the day was over before I knew it. There was no “clock-watching.” I was in a state of flow, anticipating (Dopamine) what challenge might come next, seeing it as an opportunity for continued growth.
It was a fulfilling experience, one that instilled pride and a sense of belonging — reminding me of college, with its diversity and freedom to carve a path of my own where something new to learn and experience awaited around every corner.
More importantly, I knew what I was working on had meaning, not just to myself, or the company, for that matter. The scientific and engineering world was watching to see how the project would unfold in an attempt at solving an incredibly complex problem.

The acknowledgements of my contributions extended from numerous recognitions to being asked for by name to participate in supporting programs, including Six Sigma, where I eventually was approached about becoming a Black Belt, Lessons Learned, Tenant Manager, chairing the cross-functional weekly meetings, amongst other things.
I began to notice that, when somebody came into our office, particularly Safety personnel, they bypassed the other managers or supervisors to talk with me. I believed it was more than merely being a problem-solver of sorts; I think it was because I genuinely cared about helping others, and many of the solutions I came up with benefited other organizations because of my ability to see “the bigger picture,” and forge alliances by demonstrating a gift of pattern recognition (Dopamine) — of not only seeing systems clearly, but people, too.
A corporate manager from headquarters with oversight of Bechtel National’s Office and Administrative Services, charged with overseeing employees and their career growth, was informed she needed to speak with me while on her trip to our facilities. When we met, she remarked that she had heard many positive things about me and was impressed. The meeting ended with her asking a favor: if, for any reason, I ever saw myself unhappy or thinking about leaving, to afford her the opportunity of an email or phone call to discuss it first.
Suddenly, I had what very few other people had, and even fewer people knew about, if at all, on the project: I had “The Bat Signal” to corporate. About 1.5 to two years later, I used it after I had taken on responsibilities from a position that wasn’t backfilled, and its requisition was canceled. My feeling was, in addition to Six Sigma and all these other things I was juggling, that a year was nearing since I assumed responsibilities of it, too, and that became the threshold. If I reached a year, it would be normalized, expected, and unacknowledged that I absorb those duties.
So, I used the Bat Signal and sent an email.
I received a response within 15 minutes, asking me to give her a little time to see what she could do. A day and a half later, my manager excitedly came out of his office and told me to “Dust off that old requisition!” and that it had been approved. He didn’t know how. Neither did his boss. Nevertheless, that very well may have been the highest demonstration of my value ever expressed, and that my caring had been reciprocated to the degree and level it was.
I hadn’t just achieved a bunch of accolades for the improvements I made — I established something more valuable: trust, faith, and the earned value from a powerful connection who just moved a mountain for me where others couldn’t.
The true measure of the ‘Romantic‘ element at a personal level on the YMP, however, was found not in the moment of doing something, but rather the feeling it left behind: a profound sense of pride. I recall being summoned to the General Manager’s office—a new leader who had only been on-site a few months—to plan a milestone safety event. Standing there, balancing the logistics of a Las Vegas summer against the vulnerability of a workforce with an average age of 55, I didn’t just offer locations; I offered a narrative of care. I gave him the ‘Why’ behind the precautions I offered, unsolicited.
Minutes after returning to my office, my boss walked in, his face lit with a smile that I can only describe as ‘demonstrative pride.’ He had just received a call from the GM’s office: they were impressed not just with the plan, but with the perspective. In that moment, the ‘Classicism’ of my planning and the ‘Romanticism‘ of my intuition had converged into a single, visible instance of Quality. My success was shared with my manager, who beamed, “That’s what people at that level look for. Great job!”
That was merely the set-up. The payoff occurred when, on that hot day and mindful of the conditions, the GM planned for a moment in his speech to publicly thank my crew and me for putting safety first; it was the ultimate reciprocation. It was a demonstration that when you care for the organization and its people within it, they will care for you in return.
In 2009, the Yucca Mountain Project all but closed despite decades of bipartisan support for the nation’s need to develop a nuclear spent-fuel repository, as the winds of change aligned partisan forces to usurp congressional funding requirements. Some of the top engineers and scientists, whose progress was being watched by the rest of the world, were effectively thrown under the bus and told, “We can do better.”
There was no plan. No path forward. Only “Not in my backyard,” with the hope that somebody, some state, would graciously accept nuclear waste with arms open wide. Sixteen years later, and after countless lawsuits, the nation’s problem persists, with no resolution in sight, despite the growing desire for new nuclear facilities as a cost-effective and environmentally friendly way to counter climate change.
In late 2012, after returning to New York two years prior, I received a call from somebody at the Bechtel Corporate office. They had asked for a copy of my latest résumé to “kick around.” I provided one with little thought of a response. A few months later, I was contacted yet again, strongly urged to apply for a position in their Reston, Virginia office.
I am not sure exactly what, or why, after that, as to what happened: I was contacted by someone in HR in the Reston office and effectively screened out of the process. No interview. No notification of no longer being considered for the position. No explanation for the “disconnect.” The only thing received from the HR representative on the other end of the screening phone call was:
“With all these things you’re passionate about, I just wonder if you would have any passion left for Bechtel.”
The dissonance that resulted was long-lasting. An itch that couldn’t be scratched, but somewhat relieved by the notion that someone at the corporate office had thought enough of me through the grapevine to reach out. The loop was never closed on their end, but, as part of this “recursive” process, in looking back, it’s being closed by me now.
As for the connection of the “Bat Signal,” as part of this process, I decided to see what became of her: sadly, she had passed away at the age of 77 in 2021. Her obituary stated she had retired from Bechtel in 2005, not very long after I used the signal, which explains the loss of contact.
That loss of connection was also a bit of a harbinger — an omen of sorts — that has become all too common now in the modern workplace. Something that Pirsig warned about years earlier: more technologically advanced, we would lose the ability to “care,” leading to a world of “blind, ugly things” created by unfeeling systems.
That, unfortunately, exemplifies many current hiring practices, but what happens when “care” is absent throughout an entire organization or company? I was about to see the Unified Theory play out again — only this time in its darker half, where the narrative collapses, Quality recedes, and the stumbles no longer prevent the falls.
When I walked into a food manufacturing plant in June of 2018, I experienced a level of dissonance like no other, and the feeling from their end was undoubtedly mutual.
It began in orientation at a “Leading Snack Meats Manufacturer in the Midwest” with words I never thought I would hear from a safety professional.
The company’s Safety Manager told a room full of new employees:
“I don’t believe all accidents are preventable.”
This stood in complete contrast to what had been ingrained in me and what I had helped achieve on a project with far larger stakes. It also stood in direct contrast to what the Plant Manager would later tell employees in town halls:
“My management team and I believe all accidents are preventable.”
The dissonance between those two statements was profound — and, evidently, invisible to leadership.
Before that day in orientation ended, I found a way to probe it: the conference room we were sitting in had no posted occupancy limit. I had never encountered that before and used it as an opening for discussion. The response was illuminating . . . and for all the wrong reasons.
The Safety Manager began counting ceiling tiles — a shorthand method to estimate square footage — noting that several recent town halls may have exceeded safe capacity. After estimating a number, he rationalized the absence of signage by saying that ultimately it was up to the Fire Marshal whether it was required.
That answer revealed everything.
Where I came from, safety meant anticipating risks and mitigating them before they became issues. “An ounce of prevention is worth a pound of cure.”
Here, Safety appeared to mean meeting minimum requirements without care. Just because something was not required did not mean it should not be done. That distinction, between compliance and care, would define the entire experience.
Ironically, when COVID arrived, even the water fountains suddenly had occupancy limits posted.
The dissonance in me was present from day one and would become a throughline in the narrative that followed: through management failures, quality breakdowns, and, eventually, what increasingly felt like an inevitability.
By the time I received my 60-day review, it was clear that my presence was not only experiencing dissonance, but creating it — and that change, however small, was not necessarily welcome.
My supervisor pulled me into another office, away from the bullpen where the leads, supervisors, and production manager worked. It was one of the few moments in my time there that exuded care in an unexpected context: a warning.
She told me everything was fine and that she appreciated what I had done so far, but added:
“Because of your experience, your knowledge, and the way you see things — especially safety — you can come across as very intimidating. And some people don’t like that.”
That statement explained more than she realized. Within the first 60 days, I had already encountered something that would define the culture.
A lead was sending employees on break during mandatory computer-based training, while others provided answers for them. The behavior was so brazen that it suggested not just misconduct, but comfort — the kind that only develops in an environment where accountability has eroded.
I noticed tension between this lead and the supervisor previously. The disrespect he displayed behind her back suggested she lacked authority over him, and, as it turned out, she was relatively new in her position.
I did not trust that reporting it through that channel would result in action. Talk on the floor after the training showed an unwillingness — no, a defeatedness — by others to take action. So I went directly to Human Resources and brought another employee with me to corroborate what we had experienced.
The result was immediate: suspension, followed by termination. I later learned there had been a long history of complaints about him that had never resulted in action because no one had been able to provide something “actionable” enough to overcome the fear of retaliation.
Afterward, two grown men told me they had often gone home and cried at night because of the way they had been treated. For them, the issue had never been whether they should go to HR. It was whether they trusted that doing so would make things better — or worse.
I did it because I trusted the HR manager to do the right thing.
Word eventually spread. Coworkers who had been distant, even suspicious, became warmer. Over time, quiet “thank yous” followed me on the floor. Not for reporting someone. For unwavering courage to do it. For responsible behavior and concern for others. And for leadership in the face of mediocrity.
As it turned out, trust was not one of the company’s stated values. Respect was. Respect for others and their capabilities.
During an interview with one of the Production Managers, I pointed this out after having read Paul Zak’s work on trust in organizations.
“It’s there, isn’t it?” he asked, checking. “No,” he said, surprised. “You’re right.”
I replied, “Without trust, you have nothing. I can respect you because you’re in a position of authority. That doesn’t mean I trust you to do what’s right — or to care.”
He then admitted that I was noticed by him in orientation when he did his presentation, stating, “This one here is not like the others,” and that I had a presence about me when I walked into a room. “We just need to get more management eyes on you.”
Several months later, he encouraged me to apply for a position on the third shift.
In a separate interview, the Plant Manager asked why I had applied for the job.
“To make a difference,” I said.
“Well, everyone has the opportunity to make a difference here every day.”
It was my first inkling that résumés were not being read. I pivoted to where I could demonstrate a problem: I mentioned that I had submitted nearly two dozen work orders since starting, but had no idea what happened to them.
“Somebody should be following up with you every time,” he stated.
“Not once,” I said. “Like they disappear into a black hole.” Then I told him that people stop investing time and effort into processes when they’re no longer working — the point being, not only does trust disappear into that black hole, but the respect for the individual attempting to make a value-added contribution to that very process.
He nodded and said they had recently discovered a stack of nearly two hundred work orders in a maintenance employee’s desk. That employee had since been demoted.
I couldn’t help but wonder if he had his own story — one where he, too, had stopped believing the system worked. The next ticket I submitted, the maintenance manager sought me out personally to explain what would be done and when.
For a moment, the needle moved. Then it snapped back. A new Production Manager arrived from another facility. In her first meeting with the second shift, an opportunity to build trust quietly vanished.
Employees raised a long-standing concern: the first shift had more leadership, more structure, and a fixed schedule. Second shift covered both lines, absorbed the shortfalls, and paid for it in overtime.
She raised a hand, stating, “We’re ALL ONE TEAM.” She wasn’t wrong. She just wasn’t listening. She saw the organization as it existed on paper, not the one speaking to her from the floor. What she was hearing was its engine sputtering — and she waved it off.
Not long after, I interviewed with her for a role as Process Lead that would have made use of my Six Sigma certification. Sometime later, I was unexpectedly called into the training room. The Plant Manager, QA Manager, and HR were seated inside.
“Do you know why you’re here?” the Plant Manager asked.
“No.”
“Congratulations. You’re one of two finalists for Process Lead.”
No one had told me, and when offered, I declined rescheduling the interview. I knew the routine very well by this point.
During the interview, I described a recent breakdown: a simple administrative control — verifying a scale with a one-pound weight — had lost its meaning. The scale had been off by a tenth of a pound. Over 220 pounds of ingredients, which became a 20-pound error that went unnoticed for weeks. The cost was a substantial loss of production (a batch that could be accomplished in four minutes was now taking up to nearly twenty-five minutes to complete).
The QA Manager nodded at these details, and for good reason: she was previously the Production Manager over this area.
Then I said something without realizing how telling it was at the time: I said I had recently talked with “Your Corporate Safety Manager.” The pronoun slipped out before I could catch it.
The Plant Manager corrected me. “Our Corporate Safety Manager.”
“Yes,” I replied. He was correct. It just didn’t feel that way.
I didn’t get the position; it went to a very capable individual who was already the lead on first shift and had the benefit of working on that line every day, demonstrating his value.
The Production Manager, who had waited outside in the hallway after my interview with the Plant Manager and team, to apologize and take responsibility for the lack of communication, later said, “I was so very impressed with you in your interview. We’ve got a diamond in the rough here. We need to find something more fitting for your skills.”
The sentiment was appreciated, but it had been expressed by others, from the “Trust” Production Manager to the Employee Relations Manager, who stopped by to talk to me one afternoon, telling me that management had been exploring ideas — yet nothing ever materialized.
I did, however, find myself rewriting the plant’s JSAs. This led to my meeting the Corporate Safety Manager one evening while he was visiting. I just happened to be the only person in the Safety Office when he was exiting one evening, and struck up a conversation.
After asking what I did there, and explaining to him my background, he stopped me ten minutes into a forty-minute conversation and said:
“What. The hell. Are you doing, sitting here in some cubicle in the back of an office?”
He then proceeded to do something nobody else there had: he picked my brain.
“Were your documents and safety plans ‘living documents,’ or were they created and then filed away?”
He was touching upon perhaps the most fundamental difference between my prior experience and what was exemplified here, and that his asking meant he was well aware of the current situation.
I used the example of what they had called “Playbooks,” which each department created as a broad guide for operations. Unfortunately, they neither documented complete processes nor all the hazards. There appeared to be no formal process for updating them, no Lessons Learned, such as the scale weight verification.
In one case, I approached the Production Manager (before she became QA Manager) and advocated for a safety call-out that was deleted by a supervisor to be reinstated, as it was the only place, other than the JSAs, where the safety issue was called out. She had agreed that it should be included. The “Quality Control” of the document itself was never addressed.
Ironically, the “Trust” Production Manager had earlier confided to me that the creation of these Playbooks merely felt like a formality, a box that needed to be checked.
We also discussed how Safety and Quality don’t have to be mutually exclusive, that Quality should be built into the safety processes for continuous improvement.
In many cases, processes, in general, lacked just that: Quality. I explained how, on the YMP, I did things a little differently than most: I mapped out procedures and processes. This ensured there were no “dead-ends.”
This was building Quality into processes, including Safety, as they all should be definable, measurable, repeatable, and with an expected outcome, which was clearly not happening here, even on the production floor.
At the end of the conversation, the Corporate Safety Manager asked if it would be ok for him to give the Plant Manager my name. “I believe his heart is in the right place,” he had said before adding that he should talk with me.
I was more than agreeable; I saw it as an opportunity to move the needle once again.
The Corporate Safety Manager concluded by thanking me for my time and the discussion, and that he hoped to see me somewhere more fitting on his next visit.
The Plant Manager never called on me for a discussion, and a pattern was clearly becoming more visible, one that, unfortunately, included good intentions.
In the following weeks, an incident with safety and health implications occurred that resulted in an employee voicing their displeasure at my not having been listened to, forcing management to make a move.
Once again, I was in the Safety Office when I was asked to visit the “backline” in the bakery, where an employee had returned to work after a short absence. There was some concern as to whether he should have, and I was asked to check on him.
I was very familiar with him, and regularly sought him out at the end of the shift to see if he needed a ride home — especially during the winter. After talking with him for a few moments, it was clearly evident to me that he shouldn’t be at work. Where he needed to be was in a hospital.
After expressing this to the Lead, who asked me to check on him, I then sought out the shift Supervisor and informed him of my opinion. I say this, acknowledging I had no idea what was wrong, but that it was potentially serious.
“Well . . . Is there anything light we can have him do?”
I relayed this to the Lead, telling her that, for the record, I absolutely disagreed as the employee was sent to complete computer-based training. As we passed one another, he stated, “Man, this sucks.”
Some time later, a member of the Emergency Response Team convinced the employee, after much effort, to be transported to the emergency room by ambulance. Later that night, as the shift was nearing its end, the Lead had informed me she had received an update.
“He had a stroke.”
Word had apparently gotten around that I had said he needed to be in the hospital, but that he was sent off to do training instead. The next day, someone marched into the office and let it be known that it was unacceptable.
Before long, the shift Supervisor was having a farewell luncheon and was transferring to another plant. He confided that it wasn’t by choice, that he was told to “start looking,” and that there were some incidents in which he was told by management that he failed to act “aggressively” enough.
The buck didn’t stop there. It moved—quietly, efficiently—until it disappeared.
Like the work orders. Like the warnings.
It was a stumble. But this time, no one stopped to ask what it meant. Nothing here broke all at once. It unraveled in pieces — each one small enough to ignore, until together they weren’t.
By then, I wasn’t just seeing the pattern. I was inside it.
In the spring and early summer of 2019, the plant was under a resurgence of interest in unionization. The Plant Manager, and current HR Manager, were, in part, brought there to turn the plant around, which they had, that involved quelling a unionization effort.
With the renewed attempts, communications were sent to employees’ home addresses stating why management didn’t believe unionization was warranted. One of those reasons was “We do not force you to work overtime.” It was strictly voluntary.
Meanwhile, the department itself was changing. One employee had congratulated me on becoming the new lead for the back line in the bakery. I informed her of being misinformed, that I had never applied for the position. She suddenly appeared disappointed, and evidently knew who did.
The next day, I saw her quietly stop at the job posting board in the main hallway and bid on another department.
The previous Lead, who transferred to another building, embodied the principle of “care,” as demonstrated by seeking assistance for the employee who had suffered a stroke, would not be so easily replaced.
By late 2020, after the onset of COVID, overtime had increasingly become mandatory. First, it was a few hours on Saturdays every other week. That progressed to a full shift. Then every weekend.
Before Christmas, I met with the new HR Manager to voice my concerns, based on what I was seeing and hearing. I brought up the dissonance between what was said only in the previous calendar year, the reality of the moment, what had happened in between, and what I saw happening as a result.
COVID resulted in a policy under which, if an employee came into contact with someone diagnosed with the virus, they were required to take a week off. The CARES Act temporarily altered the equation. In states like Ohio, weekly unemployment benefits, combined with the federal supplement, could significantly exceed a standard paycheck.
This created financial incentives that, for some, outweighed the cost of staying home. It wasn’t just happening at this plant, and it came with hidden costs.
As I explained to the HR Manager, everyone was aware of what was going on — as was she. The problem, I said, was that the good employees, the ones who show up every day, not only see it, they feel it.
Every time someone calls off.
Every time they have to train a new employee, only to see them leave.
Every time they’re asked to do more.
Every time overtime stops being a request and becomes required.
“It’s unsustainable. People are going to first go quiet. Then they’re going to start leaving. And then the risks are going to start increasing.” I pointed out that the overtime policy change had never been officially addressed.
As the authors of Crucial Conversations observed, when trust breaks down, people retreat into either Silence or Violence. I was watching the silence set in; the slow retreat of the plant’s best people into a state of quiet disengagement, and I knew the “violence” of a systemic collapse was the only thing left on the horizon.
I then brought up that all of this together was creating the conditions for unionization efforts to swell once again.
“I don’t know what to say.”
“I felt like you should know,” is where I left it. At least for a few weeks, until events led me to go straight to the Plant Manager in January. Twice.
“If I were the owner of this company, I would not be pleased with what I witnessed last night.”
Those were the words I used to start the conversation with. That seemed to grab his attention, as one of the company’s mantras was to think like a business owner.
What I then described to him was an Ouroboros — a snake eating its own tail. One line in the “Leading Snack Meats Manufacturer in the Midwest” had finished and cleaned up shortly after 11 p.m., only to be called back moments later to run more product.
This entailed setting the line back up, which took approximately 20 minutes, about the same amount of time to ready it for Sanitation to clean. The line was then operated for an additional hour or so, followed by another 20 minutes of preparing it for Sanitation.
The result: nearly two hours of overtime pay for roughly one hour of production. The pallet logs for the next day showed the first shift hadn’t completed a full pallet until nearly two and a half hours into their shift.
It was quickly learned that the first shift had no product to run to start the shift, because the second shift ran it the night before. Now, instead of having one line paid for two hours of overtime for one hour of work, the scenario was compounded by the first shift getting paid for no productivity.
What made it worse is that this wasn’t unusual. Morning inactivity on the first shift was becoming routine. The longer the second shift stayed, the further they cut into Sanitation’s time to do their job.
This, in turn, caused Sanitation to run into the first shift’s production time, which meant more overtime on their behalf, too, while the first shift continued to get paid to do very little other than wait in the break room.
And yet, the waste wasn’t my biggest concern. It was the employees’ mindset — and, ultimately, their safety. Frustration was causing attention to wander in an environment that already had a weak incident reporting system — one that should have been catching stumbles before they became falls.
Several days later, the “Diamond in the Rough” Production Manager approached me and informed me that the Plant Manager asked for her and me to meet, and that the shift Supervisor was coming along.
My initial thought wasn’t about the needle moving in the right direction. It was why bother? I didn’t understand what value there was in discussing it with her — unless this was for her. A test of sorts. Nevertheless, it didn’t stop me from trying.
In the meeting, I expressed the sentiments I shared with the Plant Manager and Shift Supervisor, telling them that we were overdue for a serious accident. The continued overtime, turnover, and other factors were making it inevitable. The “Risk Rating” for the plant, meanwhile, never changed. I pleaded that, at the very least, it should be elevated for the second shift.
About 20 minutes into the meeting, the Production Manager had a phone call and excused herself. The Shift Supervisor said he agreed with just about everything I said, and that the overtime needed to stop.
The only thing that stopped was the conversation. Another loop left open. Another concern swallowed by the black hole.
The exodus, as predicted, slowly began in the months that followed. By spring 2021, the company that was known for not wanting employees back if they left the job was suddenly calling those who did, offering them more to come back.
Corporate HR was now onsite, visiting building 2, where many of the skilled labor, machine operators in particular, had left. They were out there, trying to find out why.
Meanwhile, the leadership team, comprised of management and subordinates down to the supervisor level, was huddled in the training room, brainstorming. A new building had opened up, and they were unable to get two full shifts operating.
A new strategy emerged: job candidates were given a tour of the work areas before orientation. Too many were spending a week being given presentations by management, only to get out onto the production floor to find the dissonance too much.
Many went on their first and last lunch break, choosing not to return.
I continued to show up each day, applying for positions, only to see them all go to someone with seniority. Finally, a full-time position in the safety department opened up. The subsequent two interviews, held back-to-back, would be my last there.
The first, involving the Safety Manager and the full-time Safety Lead who was taking over the first shift duties, began with the Safety Manager asking, “Where did you learn about risk management? In the military?”
Later that week, discussing the interview with the Safety Lead, whom I had worked closely with, I asked, “You know where the answer to that was, right?”
“Oh, yeah,” she said, then followed with, “You’ve done a LOT.”
The answer was, in the Executive Summary, right below the contact information. Its sole purpose for being there was for a quick overview in case the reader was pressed for time.
While the first interview went well, the second posed a challenge: one of the newly anointed Production Managers was present, along with the “Diamond in the Rough” Production Manager and a third, yet to have arrived.
I had anticipated I would be treading sensitive territory, that I’d be asked about what changes I would make and the plethora of instances I had to draw from fell underneath her. And yet, at this point, I felt like Ellis Boyd “Red” Redding in The Shawshank Redemption at his third parole hearing — no longer willing to toe the line and tell the parole board what he thought they wanted to hear, but the unfiltered truth he needed to speak.
I decided to do something out of the ordinary: while we were still awaiting the third person to show, I would address it directly, but subtly, planting the seeds.
I said, “I’m sure I’m not telling you anything you don’t already know, but I’ve always found it interesting how an interviewee can discern the issues in an organization by the questions being asked.”
When the third person arrived fifteen minutes late, a new Production Manager who had been here a short time, all I could think about was how I had worked on a campus of 15 buildings and nearly 2,000 employees on both sides of a major thoroughfare, and not once in 12 years, with all the meetings and interviews I had been in and conducted, was I ever late once.
There was no apology. There was no introduction. There was no respect for my or anyone else’s time. There was, cumulatively demonstrated, no professionalism, and in that moment, I decided to become Red.
When asked my thoughts on the current status of Safety and Health in the company, I said, they talk the talk, but don’t walk it. I then proceeded to give examples within the “Diamond in the Rough” Production Manager’s department, before directing my attention to her, acknowledging that I had gone through her to address some of these issues previously.
I did this in a frank manner because at this point, I wasn’t so much interested in the position; I was interested in getting my point across, loud and clear.
A few days later, I was called into the Safety Manager’s office and told I didn’t make it to the next round of interviews. He brought up the Production Manager’s concern that she “Couldn’t possibly approve” of my advancement after that interview.
He then coached me, telling me that the right thing to do would have been to approach management and say, “I recognize a problem. I want to be part of the solution.”
If he only knew.
After a long discussion, he said there would be other opportunities coming — he had approval to hire a Supervisor to lessen his load — and that he would inform the Production Manager that we had this discussion, and that I would seek her out to have one with her as well.
I never did. There was no point. I knew what had clearly just happened. The culture I came from, this was absolutely intolerable and would have resulted in her immediate removal. Here, it was accepted. The Safety Manager even said he, unlike some others, thought she was a good manager.
It no longer mattered to me. Not only did I know this, but I had finally realized what several coworkers had told me: “You’re too good for this place.”
Some time later, another coworker informed me that the “Diamond in the Rough” Production Manager, whom he talked regularly with, was told to start looking.
“You called that one,” he said.
“I did?”
“Yeah. A few months ago. You said you didn’t see her being here much longer.”
He was right. I had forgotten I had said that. He then told me that, when she was hired, she was given three goals. In two years, she accomplished none of them.
I then made another prediction to him: the Plant Manager wouldn’t be there too much longer, either. As that turned out, I was eleven months off — but not before the inevitable happened.
It was mid to late spring when the goalposts for overtime were about to shift yet again. Now, it was a mandatory 13/1 schedule: thirteen days on, one day off. Where overtime was once voluntary, it was about to reach the 70 hours a week total for the second shift.
The company, fearing absenteeism and more employees leaving altogether while still not having a fully operating second shift in the new building, decided to incentivize perfect attendance. A monetary bonus was added to those who worked the full schedule.
I looked at the calendar and circled my last day, which would be the end of the very first week this new policy went into effect. It was just a matter of time before I submitted my two-week notice.
This is when word began spreading that there was a gruesome accident in building two. A QA person had his hand caught in a pinch point in a palletizer. The details were vague and the questions many: What happened? How? What was he doing near the equipment?
Word was, he had lost part of his hand, including a few fingers. A fellow QA employee assigned to our department talked to me about it and asked if I was squeamish before showing what the victim had posted to their own social media page, which required acknowledgment of the blurry photo’s sensitive nature.
I wasn’t privy to the accident investigation. I don’t know what contributing factors were found. I don’t know what, if any, corrective actions were taken as a result.
What I did know: I saw the photo, and it was indeed gruesome.
More importantly, I knew the accident could have been prevented.
That’s all I needed to know.
A couple of days later, the accident prompted a short “stoppage of work” for our Shift Supervisor to address it. A life-altering disfigurement was reduced to a 5 to 10-minute discussion on the need to remain focused on the task at hand.
The irony may have created its own new level of dissonance.
A few weeks later, I finally put in my two-week notice via email. The HR Specialist asked that I come in the following day early, and we briefly discussed it. He said he would contact me before the two weeks were up to conduct an exit interview.
It never happened.
I had yet to tell any coworkers, when, in the middle of a conversation I wasn’t privy to, one turned to me and said, “Jim would make a good Union President.”
Sorry, Charlie (not his name), that ship is set to sail.
The last day came, a Sunday. I did my work as I typically did — as if I were doing a marathon workout session — helping wherever I could. There was an extra pep in my step as the last hour drew near.
Upon punching out, I said my goodbyes to a few employees who hadn’t already contacted me. As I approached the security gate, I felt a certain weightlessness in my stride as the sun was beginning to set.
I’m sure my face looked like Red’s, sticking out the window of the bus with the sun on his face at the end of The Shawshank Redemption. I may have even whispered the same word as I crossed the security threshold.
“Zihuatanejo.”
When I began writing what would become the Unified Theory, I wasn’t trying to build a theory at all. I was following an intuition I didn’t yet understand.
Over time, the pattern revealed itself — first in my fiction, then in my thinking, and finally in places I never expected to find it: in real events, in real people, in real consequences.
I knew, before I left that plant, that I would someday write about what happened there. I just didn’t know how. I didn’t yet have the framework to hold it.
Looking back now, I can see that the framework was being built long before I recognized it — through a novel, through years of thought, through an idea about Pirsig and management that had been sitting quietly for nearly two decades.
None of it came from a textbook. It came from grit and living through things that didn’t make sense at the time.
Quality, in the Pirsigian sense, is never finished. It evolves as we do — as will this theory. What once felt like failure can, with time and distance, reveal itself as something else entirely.
We don’t always control what happens to us. But we do have a say in how the next chapter is written.
And remember: the more you look, the more you see.
